Federal Statutes And Regulations
- 1 Federal Statutes And Regulations —
- 2 What you’ll learn —
- 3 Blueprint mapping —
- 4 Why it matters —
- 5 Key Terms & Must-Know Facts —
- 6 Key terms —
- 7 Must-know facts —
- 8 Core content —
- 9 1.1.1.1 Foundational legal hierarchy: choose the controlling source first —
- 10 1.1.1.2 CSA versus FDCA: choose the right federal statute —
- 11 1.1.1.3 Statutes create authority; regulations implement details —
- 12 1.1.1.4 Guidance, policy, and enforcement discretion: useful but not controlling law —
- 13 1.1.1.5 Federal law on the MPJE: build the issue-spotting workflow you will use with Hawai —
Why it matters
- MPJE stems often hide the real task: not “What is good practice?” but “What source of law controls this action?”
- A common wrong answer treats guidance, policy manuals, or agency commentary as if they carry the same force as statutes or regulations.
- Federal law questions frequently pivot on the scope of the FDCA versus the CSA; choosing the wrong statute leads to the wrong agency and wrong rule set.
- This topic is the foundation for later crosswalk work with Hawaii law, where the pharmacist must satisfy both systems when both apply.
Key Terms & Must-Know Facts
1.1.1.1 Key terms
- Statute: Law enacted by Congress.
- Regulation: Binding rule issued by an agency under statutory authority.
- Guidance: Agency interpretation or recommendation; generally not binding like a statute or regulation.
- CSA: Controlled Substances Act; core federal controlled substance law.
- FDCA: Federal Food, Drug, and Cosmetic Act; core federal drug product law.
- DEA: Drug Enforcement Administration; enforces federal controlled substance law.
- FDA: Food and Drug Administration; regulates approval, labeling, and misbranding under product law.
- Delegated authority: Power given by Congress to an agency to implement details through regulations.
- Code of Federal Regulations (CFR): Published federal regulations.
- United States Code (U.S.C.): Published federal statutes.
- Misbranding: FDCA concept involving labeling or related statutory defects.
- Scheduling: CSA system for classifying controlled substances.
- Registration: DEA authorization required for controlled substance handling roles covered by federal law.
- Enforcement discretion: Agency decision about how to prioritize enforcement; not a substitute for legal permission.
1.1.1.2 Must-know facts
- Statutes create authority; regulations fill in operational detail.
- Guidance may inform compliance but does not replace controlling law.
- CSA questions usually point toward DEA authority and controlled substance handling.
- FDCA questions usually point toward FDA authority and drug approval/labeling/misbranding.
- If a stem asks what is required by law, start with statute and regulation before considering guidance.
- On MPJE, agency role confusion is a major distractor.
- Federal legality does not automatically make an action lawful under Hawaii law.
- When both federal and state law apply, the pharmacist must satisfy both; later lessons build the stricter-or-more-specific framework.
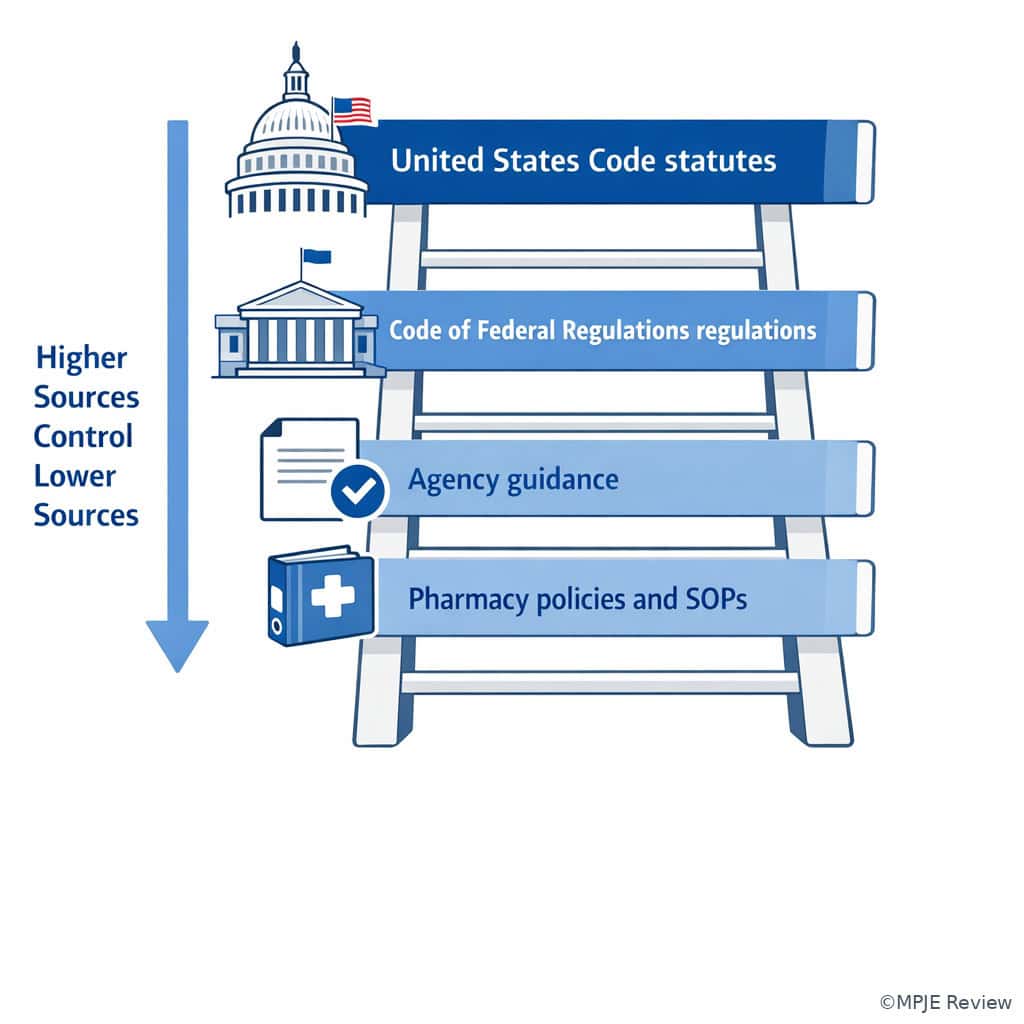
Exam takeaway: Start with the highest controlling source before relying on agency interpretations or workplace policy.
flowchart TD A[Congress enacts statute] --> B[Agency receives delegated authority] B --> C[Agency issues regulations in CFR] C --> D[Agency publishes guidance and policy] D --> E[Employer policies and SOPs] A --- F[Highest legal authority in this chain] C --- G[Binding operational detail] D --- H[Useful but not equal to law]
Exam takeaway: Visually separate statutes, regulations, guidance, and pharmacy SOPs so you do not overvalue nonbinding materials.
Core content
1.1.1.3 Foundational legal hierarchy: choose the controlling source first
A Explanation
In a federal pharmacy law stem, the first decision conflict is whether the question is asking for a legal requirement, an agency-implemented detail, or a best-practice recommendation. The resolving rule is simple: if the question asks what is required, prohibited, or legally permitted, begin with the statute and then the regulation. Guidance can explain agency thinking, but it does not create the same kind of binding duty as the underlying law. This is why See Fig 1 matters early in your workflow.
WHY THIS IS TESTED: MPJE writers frequently place an appealing answer choice that sounds authoritative because it cites a memo, manual, policy, or guidance document. The examinee must reject that choice when the stem asks for controlling law. Choose the answer grounded in the statute/regulation hierarchy; reject the answer that relies only on a recommendation or internal workflow document.
Use a three-part screen: (1) What source is being invoked? (2) Does that source have binding force for this issue? (3) Is the issue within federal product law, federal controlled substance law, or both? If a pharmacy SOP conflicts with federal regulation, the SOP cannot override the regulation. If guidance suggests a compliance approach, it may be helpful, but a question asking “what is legally required” must still be answered from statute or regulation.
Exam takeaway: When the stem asks what is legally required, escalate from policy to guidance to regulation to statute until you reach the controlling authority.
B Worked example
A 63-year-old patient with chronic pain, diabetes, and COPD presents to a community pharmacy with oxycodone 10 mg tablets, take 1 tablet by mouth every 6 hours as needed, quantity 28. The pharmacist also sees a corporate policy memo requiring a second pharmacist review for all opioid fills. The pharmacy is short-staffed, and a new intern says the fill is unlawful because the second review cannot be completed. The patient mentions that another store “always needs two signatures,” and the profile shows a distracting elevated A1c. The task is to determine the most appropriate next step under federal law.
Reasoning chain: Identify task: the question is about legality, not internal workflow preference. Extract key facts: controlled substance prescription; store policy requires extra review; issue is whether absence of that review makes dispensing unlawful. Apply rule: corporate policy may exceed legal minimum, but policy is not itself federal law. Eliminate distractors: the elevated A1c and COPD are noise; the other store’s habit is not controlling authority. Verify: the pharmacist must comply with applicable federal law and any employer policy, but should not confuse policy with a federal statutory prohibition. If the pharmacy cannot meet its internal policy, that is an operational/policy issue to clarify, not proof that federal law independently forbids dispensing.
C Exam trap
D Checkpoint
Question: A pharmacist receives amoxicillin 500 mg capsules, take 1 capsule by mouth three times daily for 10 days. A district memo says all antibiotic prescriptions should include diagnosis on the hard copy before dispensing. Which is the most appropriate interpretation if the stem asks what is legally required by federal law?
- The district memo is controlling because employer policy is enforceable within the pharmacy.
- Federal law requires the diagnosis on every antibiotic prescription because it improves stewardship.
- The pharmacist should first determine whether a federal statute or regulation imposes that requirement before treating the memo as controlling.
- FDA guidance on antimicrobial stewardship automatically creates a dispensing prohibition if diagnosis is missing.
- A: Tempting because policies matter operationally; wrong because enforceable workplace policy is not identical to federal legal requirement.
- B: Tempting because diagnosis can support appropriateness review; wrong because the stem asks about federal legal requirement, not best practice.
- C: Correct because the legal question must be answered from statute/regulation hierarchy first.
- D: Tempting because guidance can influence compliance; wrong because guidance alone does not automatically create a legal prohibition.
1.1.1.4 CSA versus FDCA: choose the right federal statute
A Explanation
The second foundational decision conflict is whether the issue belongs primarily to the Controlled Substances Act or the Federal Food, Drug, and Cosmetic Act. The single resolving clue is the subject matter. If the stem is about scheduling, DEA registration, ordering, inventory, dispensing limits for controlled substances, or diversion-related duties, think CSA. If the stem is about approval status, labeling, adulteration, misbranding, or product marketing/distribution status, think FDCA. See Fig 3.
WHY THIS IS TESTED: Examinees often know the fact pattern but attach it to the wrong statute. MPJE does not reward partial recognition. A question about a controlled prescription’s refill legality belongs to CSA/DEA, not FDCA/FDA. A question about whether a drug is approved, properly labeled, or misbranded belongs to FDCA/FDA, not the CSA.
Some stems contain both product-law and controlled-substance signals. In those cases, do not force a single-statute answer too early. Ask which issue the question is targeting. For example, a controlled substance may also raise labeling issues, but if the stem asks whether the pharmacy may refill it, the controlled substance framework controls that task. If the stem asks whether the product’s labeling or approval status is defective, the FDCA framework controls that task.
Exam takeaway: Match the issue in the stem to the statute before deciding which agency or rule set applies.
flowchart LR
A[Question stem] --> B{Main issue?}
B -->|Scheduling registration refills ordering inventory diversion| C[CSA]
B -->|Approval labeling misbranding adulteration product status| D[FDCA]
C --> E[DEA-centered implementation]
D --> F[FDA-centered implementation]
E --> G[Look for controlled substance rule]
F --> H[Look for product-law rule] Exam takeaway: Controlled-substance workflow cues usually point to DEA, while approval and labeling cues usually point to FDA.
B Worked example
A 44-year-old patient with ADHD and hypertension presents with methylphenidate 10 mg tablets, take 1 tablet by mouth twice daily. The pharmacist notices the manufacturer recently changed carton artwork, and a technician worries the product may be “misbranded,” while another staff member asks whether the prescription can be transferred because the patient is traveling. The patient also mentions a shellfish allergy, a tempting but irrelevant clue. The task is to identify which statute controls the transfer question.
Reasoning chain: Identify task: the question is about transfer legality for a controlled substance prescription, not carton design. Extract key facts: methylphenidate is controlled; the issue is transfer. Apply rule: controlled substance dispensing/transfer rules fall under the CSA and DEA implementation. Eliminate distractors: packaging change and possible misbranding would point toward FDCA/FDA, but that is not the question asked. Verify: use CSA/DEA authority first, then later crosswalk with state law if the stem requires both federal and Hawaii compliance.
C Exam trap
D Checkpoint
Question: A pharmacist reviews semaglutide injection 0.25 mg subcutaneously weekly and is asked whether a repackaged version lacking proper labeling may be unlawfully distributed. Which federal statute is most directly implicated?
- The CSA, because semaglutide is a prescription medication.
- The FDCA, because the issue is labeling and product status.
- The CSA, because all dispensing questions fall under DEA authority.
- Neither statute, because labeling defects are only state board issues.
- A: Tempting because many prescriptions are regulated generally; wrong because prescription status alone does not make it a CSA issue.
- B: Correct because labeling and misbranding are FDCA-centered concepts.
- C: Tempting because DEA is prominent on MPJE; wrong because DEA does not control all drug-law topics.
- D: Tempting if the learner over-localizes pharmacy regulation; wrong because federal product law directly addresses labeling issues.
- The main federal statute for controlled substance scheduling and registration is CSA.
- True or False: A labeling defect usually points first to the FDCA. True.
- Name the two agencies most often paired with these statutes: DEA and FDA.
1.1.1.5 Statutes create authority; regulations implement details
A Explanation
Once you identify the correct statute, the next decision conflict is whether the answer needs the broad legal authority or the specific operational detail. The resolving rule is: statutes establish the framework and grant agency authority; regulations translate that authority into day-to-day requirements. On the MPJE, if an answer option sounds broad and another option gives a more precise agency rule implementing that broad command, the operational rule usually wins when the question asks how a pharmacist must act in practice. See Fig 4.
WHY THIS IS TESTED: Many learners memorize act names but not how those acts become usable compliance rules. Questions often hinge on whether Congress or the agency supplied the exact detail. For example, a statute may authorize regulation of controlled substance recordkeeping, while the detailed retention, ordering, or inventory requirements are implemented in regulations. Similarly, the FDCA establishes product-law authority, but the working details may live in agency regulations and official labeling frameworks.
This distinction matters because some answer choices overclaim what the statute itself says, while others correctly identify that the statute authorized the agency to specify details by regulation. If the stem asks “where does the agency get the power to issue this rule?” think statute. If it asks “what specific operational requirement applies?” think regulation. Guidance can help interpret ambiguous points, but it is not the same category of authority.
Exam takeaway: The statute gives the agency power, but the regulation usually supplies the practice-level detail tested on MPJE.
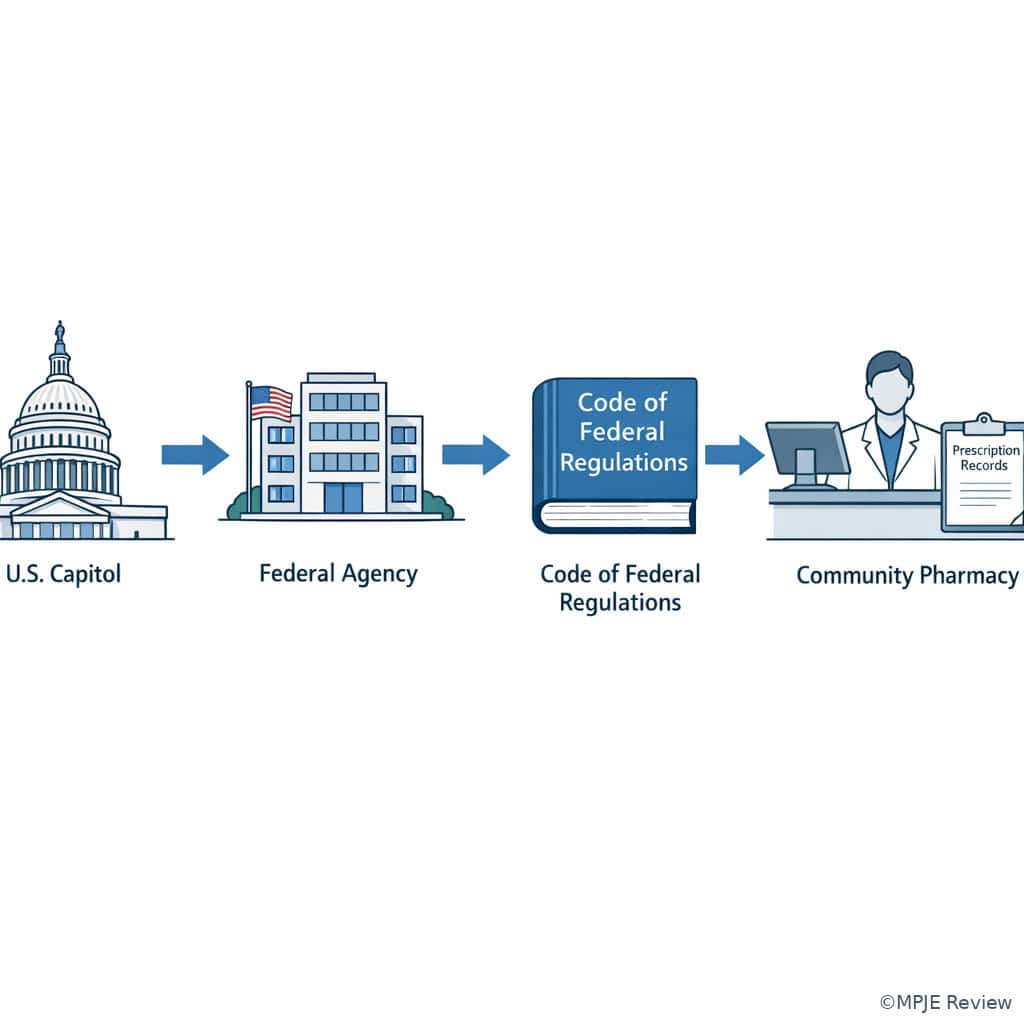
flowchart TD A[Statute enacted] --> B[Agency authority delegated] B --> C[Notice and rulemaking process] C --> D[Final regulation published] D --> E[Pharmacy compliance workflow] E --> F[Documentation inspection enforcement]
Exam takeaway: Visualizing the chain from statute to regulation helps separate broad authority from the exact operational duty in a stem.
B Worked example
A hospital pharmacist is reviewing morphine 2 mg IV every 4 hours as needed for a 71-year-old patient with cancer, CKD, and atrial fibrillation. During a DEA inspection drill, a resident asks whether the exact inventory documentation rule comes “directly from the CSA itself.” Another pharmacist argues that if the statute mentions recordkeeping broadly, no regulation is needed. The medication order and renal function are distracting clinical facts. The task is to choose the best legal explanation.
Reasoning chain: Identify task: source of detailed authority. Extract key facts: controlled substance inventory/recordkeeping question; clinical details do not change the legal source issue. Apply rule: the CSA creates the framework and authorizes DEA regulation; detailed implementation is commonly found in regulations. Eliminate distractors: the presence of a patient-specific opioid order does not convert an operational compliance question into a clinical dosing problem. Verify: answer with the statute-to-regulation structure, not with a vague statement that “the Act covers everything.”
C Exam trap
D Checkpoint
Question: A pharmacist reviewing lisdexamfetamine 30 mg by mouth every morning is asked where the detailed federal requirements for handling a controlled prescription are most likely to be implemented after Congress creates the underlying authority. Which is the best answer?
- In agency regulations issued under the statute’s delegated authority.
- Only in nonbinding guidance documents, because statutes are intentionally vague.
- Only in pharmacy corporate policies, because agencies do not regulate practice details.
- Only in state board newsletters, because federal statutes do not reach dispensing workflow.
- A: Correct because regulations supply binding operational detail under the statute.
- B: Tempting because guidance can be practical; wrong because guidance is not the primary binding implementation tool.
- C: Tempting when learners overvalue SOPs; wrong because corporate policy cannot replace federal regulations.
- D: Tempting because boards influence practice; wrong because federal law clearly reaches many pharmacy workflows.
1.1.1.6 Guidance, policy, and enforcement discretion: useful but not controlling law
A Explanation
Another recurring MPJE conflict is whether an agency statement, FAQ, compliance guide, or internal policy creates a mandatory legal rule. The single resolving principle is that guidance informs compliance but does not replace law. It may show how an agency interprets or prioritizes enforcement, and it may be highly influential in practice, but if the stem asks what is legally required, your final answer must rest on statute/regulation unless the question expressly asks about guidance or enforcement position. See Fig 5.
WHY THIS IS TESTED: These sources sound sophisticated and exam-like. A student who has seen real-world compliance documents may overread their legal status. On the MPJE, you must distinguish “helpful interpretive material” from “binding legal command.” This does not mean guidance is irrelevant. It matters when clarifying ambiguous compliance expectations, training staff, or anticipating regulator scrutiny. It just cannot substitute for the underlying source of legal authority.
Likewise, employer policy may be stricter than federal minimums. A pharmacist may still need to follow that policy as a condition of employment, but an MPJE question about federal legality is not answered by saying “because the store requires it.” The best answer will separate operational prudence from actual legal obligation.
Exam takeaway: A stem asking what is required by law should steer you away from guidance-only or policy-only answer choices.
flowchart TD
A[Source named in stem] --> B{Type of source}
B -->|Statute or regulation| C[Binding legal authority]
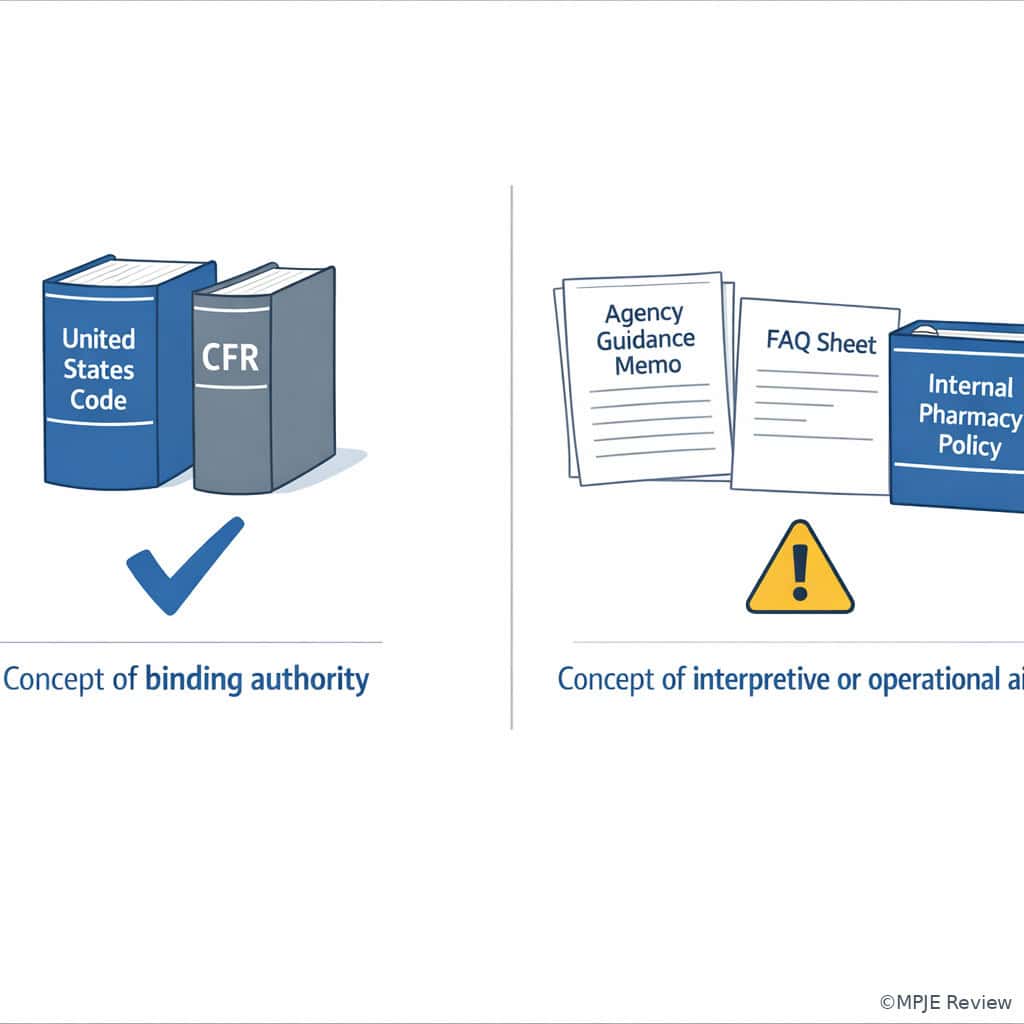
B -->|Guidance FAQ policy memo| D[Interpretive or operational aid]
C --> E[Use for lawful next step]
D --> F[Use with caution; verify law first] Exam takeaway: The visual contrast between CFR books and guidance memos helps prevent the classic “guidance equals law” mistake.
B Worked example
A 58-year-old patient with metastatic cancer, constipation, and obstructive sleep apnea presents with fentanyl transdermal 25 mcg/hour every 72 hours. A staff pharmacist cites an agency FAQ suggesting one approach to suspicious-order review, while the pharmacy’s written SOP requires an additional manager signoff for any first-time opioid pickup. A new graduate asks whether the FAQ alone makes the signoff federally required. The patient’s mildly elevated AST is distracting noise. The task is to determine the lawful interpretation.
Reasoning chain: Identify task: source status. Extract key facts: FAQ and SOP are being treated as law. Apply rule: FAQ/guidance may inform practice, and SOP may impose a workplace process, but neither automatically equals binding federal legal command. Eliminate distractors: the liver test and cancer diagnosis do not change source hierarchy. Verify: the pharmacist should comply with applicable law and workplace procedures, but must describe the source accurately and avoid stating that the FAQ independently created the duty.
C Exam trap
D Checkpoint
Question: A pharmacist is verifying insulin glargine 20 units subcutaneously nightly. An agency compliance guide recommends a documentation practice, but the stem asks which action is required by federal law. Which is the best answer?
- Follow the guide because all agency publications automatically create binding legal obligations.
- Treat the guide as helpful, but confirm whether the requirement appears in statute or regulation before calling it legally mandatory.
- Ignore the guide entirely because nonbinding sources are never relevant.
- Use the pharmacy SOP instead of federal sources because practice standards are local.
- A: Tempting because agency publications feel official; wrong because not all publications are binding law.
- B: Correct because guidance may help but cannot replace statute/regulation when the question asks what is legally required.
- C: Tempting as an overcorrection; wrong because guidance can still inform interpretation and compliance planning.
- D: Tempting in workflow-heavy environments; wrong because SOPs do not displace controlling federal law.
- True or False: Agency guidance can be useful without being the controlling law. True.
- If the stem asks what is legally required, start with statute and regulation.
- A pharmacy SOP may be stricter than law, but it does not replace law.
1.1.1.7 Federal law on the MPJE: build the issue-spotting workflow you will use with Hawaii law
A Explanation
The final foundational skill is not just naming sources but using them in the right order during a mixed-jurisdiction problem. Even though this lesson is federal-only, MPJE success depends on building a repeatable workflow now: identify the issue, identify the federal source, decide whether Hawaii law also applies, then choose the stricter or more specific lawful answer when later lessons require it. The resolving clue is the scope of the task: if the stem is purely federal, answer federally; if it signals pharmacy operations in Hawaii, prepare to crosswalk federal and state rules in later topics.
WHY THIS IS TESTED: Learners often answer too narrowly. They identify the correct federal rule but forget the exam’s core structure: federal permission does not automatically authorize conduct in Hawaii. Conversely, a Hawaii workflow cannot excuse failure to satisfy a federal controlled substance requirement. This lesson starts the first half of that two-system habit.
Use this sequence: (1) spot the issue category; (2) assign it to CSA or FDCA; (3) identify whether the answer needs statute or regulation; (4) downgrade guidance/policy if the stem asks for legal duty; (5) pause and ask whether state law must also be satisfied. Upcoming topics will supply the Hawaii side and the specific roles of the board, DEA, and FDA.
Exam takeaway: Solve the federal source question first, then check whether Hawaii law adds another controlling layer.
Exam takeaway: A visual workflow helps prevent stopping after the federal answer when the exam later expects a federal-plus-Hawaii analysis.
B Worked example
A pharmacist in Honolulu receives buprenorphine/naloxone 8 mg/2 mg films, dissolve 1 film sublingually daily, from an out-of-state prescriber for a 36-year-old patient with opioid use disorder, hepatitis C, and depression. A technician asks whether the case is “purely DEA” because the medication is controlled. Another pharmacist says Hawaii practice rules do not matter if the prescription is federally valid. The patient also requests an early fill because of travel, and the profile shows a distracting low vitamin D level. The task is to identify the best reasoning approach.
Reasoning chain: Identify task: source-and-scope workflow. Extract key facts: controlled substance means federal CSA/DEA analysis is necessary; the pharmacy is in Hawaii, so Hawaii law may also apply. Apply rule: federal analysis comes first for the controlled substance component, but it is not the end of the inquiry if state law also governs dispensing or operational requirements. Eliminate distractors: the vitamin D result and travel request may matter later but do not alter the source hierarchy. Verify: the best approach is to determine the federal rule, then crosswalk Hawaii law before concluding the lawful next step.
C Exam trap
D Checkpoint
Question: A Hawaii pharmacist is asked about a federal labeling issue for metformin 500 mg by mouth twice daily and a separate state workflow requirement for documentation. What is the best starting approach?
- Answer only under Hawaii law because the pharmacy is located in Hawaii.
- Answer only under federal law because product-law questions always preempt state workflow rules.
- Identify the federal product-law source first, then determine whether Hawaii law adds a separate controlling requirement.
- Use whichever source is easier to remember because both are equally optional on the MPJE.
- A: Tempting because state boards regulate pharmacies; wrong because federal product law still governs federal issues.
- B: Tempting because FDCA is central to labeling; wrong because the stem signals an additional Hawaii workflow requirement.
- C: Correct because MPJE reasoning requires source identification and then cross-jurisdiction checking when both systems apply.
- D: Tempting as a test-taking shortcut; wrong because the exam rewards structured legal hierarchy, not convenience.
Exam Traps & Differentiators
- Most common wrong answer and why: Treating guidance as controlling law. It is tempting because it comes from the same agency and often uses directive language.
- Looks similar but isn’t: CSA versus FDCA. Both are federal drug laws, but one governs controlled-substance handling while the other governs product approval/labeling/misbranding.
- Looks similar but isn’t: Regulation versus policy. Both can tell staff what to do, but only one is binding federal law in the legal hierarchy sense.
- Neighbor-topic confusion: Upcoming Hawaii statutes/rules may impose additional requirements, but they are not the source of federal authority for CSA or FDCA questions.
| Stem says... | Think... | Why |
|---|---|---|
| “required by federal law” | Statute or regulation first | Guidance or policy alone is not enough. |
| “schedule,” “registration,” “inventory,” “refill limit,” “transfer” | CSA / DEA lane | These are controlled-substance handling signals. |
| “approval,” “misbranding,” “adulteration,” “labeling” | FDCA / FDA lane | These are product-law signals. |
| “where does the agency get the power?” | Statute | Congress creates the authority. |
| “what exact operational rule applies?” | Regulation | Agencies implement details through regulations. |
| “FAQ,” “guidance,” “memo,” “policy” | Interpretive aid, not automatic legal command | Useful, but verify controlling law. |
| Confusable pair | Why the wrong answer is tempting | Single clue that eliminates it |
|---|---|---|
| Guidance vs regulation | Both may come from the same agency. | The source is labeled FAQ/guidance/memo rather than a binding rule. |
| CSA vs FDCA | Both involve drugs and federal agencies. | The issue is controlled handling vs product status/labeling. |
| Federal validity vs Hawaii legality | Federal law feels comprehensive. | The pharmacy is practicing in Hawaii, so state law may also govern. |
| Statute vs regulation | The named Act sounds like it contains all details. | The question asks for day-to-day operational requirements. |
If the stem says “corporate policy requires...”, think policy may matter operationally, but it is not automatically the federal legal answer.
If the stem says “DEA registration”, think CSA-centered controlled substance framework.
If the stem says “misbranding”, think FDCA-centered product-law framework.
If the stem says “in Hawaii”, think federal answer first, then Hawaii crosswalk.
If the stem says “best next step” after a source dispute, think identify the controlling legal source before acting.
Tables
| Reference point | High-yield meaning | MPJE use |
|---|---|---|
| Statute | Congress-created law | Use when the stem asks where authority comes from. |
| Regulation | Binding agency rule implementing statute | Use when the stem asks for precise operational requirements. |
| Guidance | Interpretive/compliance aid | Useful context, but do not treat as controlling law unless the question is specifically about guidance. |
| CSA | Core federal controlled substance statute | Think schedule, registration, refill/transfer, inventory, ordering, diversion. |
| FDCA | Core federal product-law statute | Think approval, labeling, misbranding, adulteration, product status. |
| DEA | Controlled-substance enforcement/implementation agency | Pair with CSA-centered tasks. |
| FDA | Product-law enforcement/implementation agency | Pair with FDCA-centered tasks. |
| Item | CSA / DEA side | FDCA / FDA side | Closest confounder |
|---|---|---|---|
| Schedule assignment | Primary lane | Not the primary lane | Product approval status |
| DEA registration | Primary lane | Not the primary lane | State board licensure |
| Prescription transfer of controlled substance | Primary lane | Not the primary lane | Prescription labeling defect |
| Misbranding | Not the primary lane | Primary lane | Controlled refill legality |
| Labeling defect | Not the primary lane | Primary lane | Registration defect |
| Adulteration | Not the primary lane | Primary lane | Diversion red flags |
| Differential question type | Best source to start with | What to reject |
|---|---|---|
| “What law authorizes this federal agency action?” | Statute | Guidance-only answer |
| “What exact federal operational duty applies?” | Regulation under that statute | Broad act name without implementation detail |
| “What does this agency FAQ recommend?” | Guidance | Calling it binding law unless supported by statute/regulation |
| “Can this controlled prescription be handled this way?” | CSA / DEA rules | FDCA-only answer |
| “Is this product mislabeled or misbranded?” | FDCA / FDA rules | CSA-only answer |
| “In Hawaii, what is the lawful next step?” | Federal source first, then Hawaii crosswalk | Stopping after one jurisdiction |
Algorithm / Approach
Rapid Review
- Statute → source of authority, not always the exact workflow detail
- Regulation → practice-level implementation of statutory authority
- Guidance → interpretive aid; do not call it controlling law unless the stem asks about guidance itself
- CSA → scheduling, registration, transfers, refills, ordering, inventory, diversion
- FDCA → approval, labeling, misbranding, adulteration, product status
- DEA → controlled-substance implementation lane
- FDA → product-law implementation lane
- Corporate policy → may be stricter than law, but not the same as federal legal authority
- FAQ/memo → tempting distractor because it sounds official
- Authority question → think statute first
- Operational-duty question → think regulation first
- Hawaii pharmacy setting → federal answer may be necessary but not sufficient
- Mixed stem with extra facts → answer the asked issue, not every issue mentioned
- MPJE source trap → the most official-sounding answer is not always the controlling one
Self-check quiz
1. A pharmacist reviews amphetamine/dextroamphetamine 10 mg by mouth twice daily for a 22-year-old patient with ADHD and asthma; the patient also takes albuterol HFA as needed and reports mild insomnia. The intern asks which federal statute most directly governs schedule-based handling and registration questions for this prescription. What is the most appropriate answer?
- Controlled Substances Act
- Federal Food, Drug, and Cosmetic Act
- Poison Prevention Packaging Act
- HIPAA Privacy Rule
2. A pharmacist verifies isotretinoin 30 mg by mouth twice daily for a 19-year-old patient with acne and depression history; the patient also uses drospirenone/ethinyl estradiol daily and ibuprofen as needed. A technician asks which federal law is the core source for approval and misbranding concepts. What is the best answer?
- Controlled Substances Act
- Federal Food, Drug, and Cosmetic Act
- Ryan Haight Act only
- Occupational Safety and Health Act
3. A community pharmacist receives oxycodone 5 mg by mouth every 6 hours as needed, quantity 20, for a 68-year-old patient with osteoarthritis, CKD, and COPD. The store policy requires dual review for all first-time opioid prescriptions, but only one pharmacist is on duty. The patient’s serum potassium of 5.2 mEq/L appears in the profile as a distracting detail. If the question asks what is required by federal law, what is the most appropriate next step?
- Conclude dispensing is federally unlawful because internal policy was not met.
- Determine the controlling federal statute or regulation before treating the policy as a legal prohibition.
- Rely on a company training slide because operational documents are the highest authority in workflow questions.
- Ignore all policies because only state law matters at the pharmacy counter.
4. A pharmacist reviews methylphenidate ER 18 mg by mouth every morning for a 14-year-old patient with ADHD and anxiety; the patient also takes sertraline 25 mg daily and cetirizine 10 mg daily. The carton design recently changed, but the stem asks whether the prescription may be transferred under federal law. Which framework is the best starting point?
- FDCA because packaging is mentioned in the stem
- CSA because the task is controlled-prescription handling
- State board newsletter because transfer questions are local only
- Employer SOP because it governs daily operations
5. A pharmacist verifies semaglutide 0.5 mg subcutaneously weekly for a 57-year-old patient with obesity, hypertension, and GERD. A wholesaler notice raises concern that a relabeled version may lack required labeling elements. The patient also uses omeprazole 20 mg daily and lisinopril 20 mg daily. If the question asks which federal statute is most directly implicated, what is the best answer?
- CSA because semaglutide is dispensed by prescription
- FDCA because the issue is labeling and possible misbranding
- CSA because all pharmacy distribution issues are controlled-substance issues
- No federal statute because labeling is only a state board matter
6. A Hawaii pharmacist is reviewing buprenorphine/naloxone 8 mg/2 mg films, 1 film sublingually daily, for a 39-year-old patient with opioid use disorder, hepatitis C, and insomnia; the patient also takes trazodone 50 mg at bedtime and ibuprofen 400 mg as needed. A staff member confirms the prescription appears federally valid and says no further legal review is needed. The patient requests early pickup for interisland travel. What is the most appropriate legal reasoning approach?
- Stop after federal review because controlled-substance questions are exclusively federal.
- Apply Hawaii law only because the dispensing pharmacy is in Hawaii.
- Identify the federal controlled-substance rule first, then determine whether Hawaii law adds additional controlling requirements.
- Follow the pharmacy SOP only because it is the most specific source available at the counter.
7. A pharmacist verifies fentanyl patch 25 mcg/hour every 72 hours for a 61-year-old patient with cancer pain, constipation, and atrial fibrillation; the patient also receives apixaban 5 mg twice daily and senna 17.2 mg nightly. An agency FAQ recommends one documentation practice, but the stem asks which action is legally required. Which answer is most appropriate?
- Treat the FAQ recommendation as binding because it came from the agency that enforces the law.
- Use the FAQ as interpretive support, but confirm the requirement in statute or regulation before calling it mandatory.
- Disregard the FAQ completely because nonbinding sources are never useful in pharmacy compliance.
- Use apixaban therapy as the deciding clue because anticoagulation changes federal source hierarchy.
8. A hospital pharmacist reviews morphine 2 mg IV every 4 hours as needed for a 73-year-old patient with metastatic cancer, CKD stage 4, and COPD; the patient also receives ondansetron 4 mg IV every 8 hours as needed and pantoprazole 40 mg IV daily. During orientation, a resident asks whether the exact federal inventory record rule exists because Congress wrote it directly into the statute or because the agency implemented it under delegated authority. What is the best answer?
- The exact practice-level detail is typically implemented through agency regulations under statutory authority.
- The exact practice-level detail can only come from internal hospital policy.
- The exact practice-level detail must come from guidance because statutes are never implemented by regulations.
- The patient’s renal impairment makes federal recordkeeping rules inapplicable to this order.
Answer key
1. Correct answer: A — Controlled Substances Act.
- A: Tempting because the medication is a stimulant with controlled-substance implications; correct because schedule-based handling and registration are classic CSA subjects, implemented through DEA authority. The single clue is the stem’s focus on schedule-based handling and registration. Source: Controlled Substances Act; DEA regulations.
- B: Tempting because the FDCA is a major federal drug law; incorrect here because approval/labeling/misbranding is not the task presented. The single clue eliminating it is that the stem asks about schedule-based handling, not product status. Source: FDCA versus CSA scope distinction.
- C: Tempting because packaging laws affect drug dispensing; incorrect because child-resistant packaging is a different federal framework and does not govern schedule classification or DEA registration. The single clue is the absence of a packaging task. Source: PPPA scope.
- D: Tempting because HIPAA appears in pharmacy law settings; incorrect because privacy law does not govern controlled-substance scheduling or registration. The single clue is that the stem concerns federal controlled handling, not disclosure. Source: HIPAA privacy framework.
2. Correct answer: B — Federal Food, Drug, and Cosmetic Act.
- A: Tempting because isotretinoin is tightly regulated in practice; incorrect because the stem asks about approval and misbranding concepts, which are FDCA-centered, not CSA-centered. The single clue is approval and misbranding. Source: FDCA product-law authority.
- B: Correct because approval, labeling, and misbranding are core FDCA subjects under FDA oversight. The single discriminating clue is the product-law terminology. Source: FDCA; FDA labeling and approval framework.
- C: Tempting because a learner may remember specific program requirements associated with certain medications; incorrect because the question asks for the core federal law governing approval/misbranding, not a narrower law or program. The single clue is the broad product-law framing. Source: FDCA as core statute.
- D: Tempting because OSHA affects pharmacy workplaces; incorrect because workplace safety does not govern approval or misbranding. The single clue is that the issue is product legal status, not employee safety. Source: OSHA scope.
3. Correct answer: B — Determine the controlling federal statute or regulation before treating the policy as a legal prohibition.
- A: Tempting because dual review policies are common and safety-oriented; incorrect because failure to meet internal policy does not itself prove a federal legal prohibition. The single clue is the stem asking what is required by federal law. Source: source hierarchy principle; statute/regulation over policy.
- B: Correct because the pharmacist must identify controlling federal law before calling a policy-based workflow a legal bar. The single clue is the explicit legal framing of the question. Source: federal hierarchy of authority; agency regulations implement details.
- C: Tempting because training slides often summarize real requirements; incorrect because summaries are not themselves the highest authority. The single clue is that a training slide is not the legal source. Source: guidance/policy distinction.
- D: Tempting as a reaction against overvaluing policy; incorrect because federal law clearly matters in many dispensing contexts. The single clue is that the prescription is oxycodone, a controlled substance with federal implications. Source: CSA applicability.
4. Correct answer: B — CSA because the task is controlled-prescription handling.
- A: Tempting because packaging changes can suggest an FDCA issue; incorrect for this scenario because the question asks about transfer legality of a controlled prescription. The single clue is may be transferred under federal law. Source: CSA/DEA transfer framework.
- B: Correct because the task is controlled-prescription handling, which falls in the CSA/DEA lane. The single clue is the operational issue of transfer. Source: CSA scope.
- C: Tempting because states regulate pharmacies; incorrect because the question asks for the best federal starting point, not local-only authority. The single clue is the phrase under federal law. Source: federal-state interaction principle.
- D: Tempting because SOPs govern daily operations; incorrect because SOPs do not decide the governing federal legal framework. The single clue is the legal source question. Source: source hierarchy principle.
5. Correct answer: B — FDCA because the issue is labeling and possible misbranding.
- A: Tempting because semaglutide is a prescription drug; incorrect because prescription status alone does not convert labeling concerns into CSA questions. The single clue is lacking required labeling elements. Source: FDCA labeling/misbranding framework.
- B: Correct because labeling defects and misbranding are product-law issues under the FDCA. The single clue is the relabeling concern. Source: FDCA; FDA product-law authority.
- C: Tempting because the pharmacy is involved in distribution; incorrect because not all distribution questions are controlled-substance questions. The single clue is the product-labeling focus rather than schedule-handling focus. Source: CSA versus FDCA differentiation.
- D: Tempting if the learner overfocuses on state boards; incorrect because federal product law directly reaches labeling issues. The single clue is the federal labeling defect. Source: FDCA scope.
6. Correct answer: C — Identify the federal controlled-substance rule first, then determine whether Hawaii law adds additional controlling requirements.
- A: Tempting because buprenorphine/naloxone is a controlled medication and federal law is central; incorrect because the pharmacy is in Hawaii, so state law may also apply. The single clue is the Hawaii pharmacist setting. Source: MPJE federal-state dual compliance framework.
- B: Tempting because the pharmacy practices in Hawaii; incorrect because controlled-substance federal law still must be satisfied. The single clue is the controlled-substance nature of the prescription. Source: CSA applicability plus state overlay concept.
- C: Correct because the best workflow is federal controlled-substance analysis first, then Hawaii crosswalk. The single clue is the combination of a controlled drug and Hawaii practice setting. Source: dual-jurisdiction compliance approach.
- D: Tempting because SOPs feel specific and practical; incorrect because specificity of workflow does not make SOPs the controlling legal source. The single clue is that the question asks for legal reasoning, not internal process preference. Source: policy versus law hierarchy.
7. Correct answer: B — Use the FAQ as interpretive support, but confirm the requirement in statute or regulation before calling it mandatory.
- A: Tempting because the FAQ came from the enforcing agency and may use directive language; incorrect because agency FAQ alone does not automatically create binding legal duty. The single clue is that the source is an FAQ. Source: guidance versus binding authority distinction.
- B: Correct because the legally required action must be traced to statute or regulation, even though the FAQ may inform interpretation. The single clue is the stem’s phrase legally required. Source: statute/regulation hierarchy; agency guidance principles.
- C: Tempting as an overcorrection; incorrect because FAQs can still help interpret expectations and enforcement posture. The single clue is that the question is about legal force, not usefulness. Source: guidance utility versus legal binding effect.
- D: Tempting because anticoagulation is a clinically important detail; incorrect because apixaban does not change the source hierarchy question. The single clue is that the clinical detail is noise unrelated to legal authority. Source: exam technique for separating legal issue from clinical noise.
8. Correct answer: A — The exact practice-level detail is typically implemented through agency regulations under statutory authority.
- A: Correct because Congress establishes authority in the statute, and the agency commonly supplies exact operational rules by regulation. The single clue is the question’s focus on exact federal inventory record rule. Source: statute-to-regulation implementation model.
- B: Tempting because hospitals often have detailed inventory policies; incorrect because internal policy cannot be the sole source of a federal recordkeeping rule. The single clue is that the resident asked about the federal rule. Source: policy versus regulation distinction.
- C: Tempting because guidance often explains documentation practices; incorrect because guidance does not replace regulations as the usual source of exact binding implementation detail. The single clue is the phrase implemented under delegated authority. Source: administrative law framework in pharmacy regulation.
- D: Tempting because CKD affects opioid pharmacotherapy; incorrect because patient renal status has no bearing on whether federal inventory rules apply. The single clue is that the issue is recordkeeping source, not dosing safety. Source: exam issue-spotting discipline.